

If you’ve woken up with a shooting, burning pain down your leg, struggled to find a position that’s even remotely comfortable, or been told by a healthcare professional that you have sciatica — you’re in very good company. It’s one of the most common things I see in clinic, and also one of the most misunderstood.
People often arrive convinced that something is seriously wrong structurally, that they need a scan urgently, that they’ll require surgery, or that the pain will simply never go away. And while I understand completely why it feels that way — sciatica can be genuinely horrendous — the vast majority of the time, none of those things are true.
This post covers everything you actually need to know: what sciatica is, what causes it, what a thorough assessment involves, what role imaging plays (and equally, when it doesn’t help), and what treatment actually looks like — including exercise, medication, and injections. Let’s get into it.
Table of Contents
What actually is sciatica?
Sciatica is a symptom, not a diagnosis. That’s an important distinction. It describes pain, and often tingling, numbness, or weakness that travels down the leg along the course of the sciatic nerve or one of its contributing nerve roots. The underlying cause of that irritation is what actually needs identifying and treating.
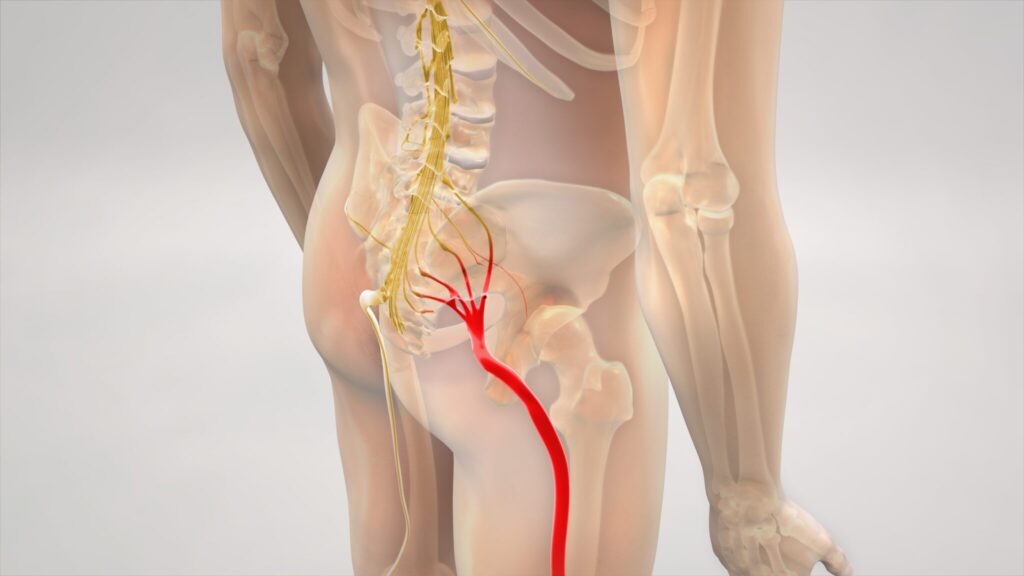
The sciatic nerve is the largest nerve in the body, up to two centimetres in diameter at its thickest point. It starts in the lower back, formed from nerve roots that exit between the vertebrae (bones) of the lumbar and sacral spine (from L4 to S3 if you want to get technical). These roots combine in the pelvis to form the sciatic nerve itself which then runs down through the back of the buttock and thigh before splitting into branches that supply the lower leg and foot.
When one of those nerve roots becomes irritated — whether by mechanical pressure, inflammation, or a combination of both — signals are sent down the nerve that you experience as pain, tingling, burning, or altered sensation in the leg. The distribution of the symptoms often gives useful clinical information about which nerve root is involved.
One thing worth flagging early on: approximately only up to 10% of back-related pain problems are truly nerve-related. Referred pain from sensitive joints, muscles, and other spinal structures can radiate convincingly into the buttock and even the leg, and can feel very similar to genuine sciatica. This is one of the reasons why a proper clinical assessment, done by someone who knows what they’re looking for is so valuable. You can’t reliably self-diagnose sciatica based on leg pain alone.
What causes sciatica?
The most common cause is a change in one of the intervertebral discs in the lower back — but before we get into what can go wrong, let’s talk briefly about what discs actually are, because a lot of the language around them causes unnecessary fear.
Discs: tougher than you've been told
Discs are robust, load-bearing structures. They sit between each pair of vertebrae and are designed to absorb force, allow movement, and maintain height in the spine. Crucially, they are firmly attached to the bones above and below them — they cannot slip, pop out, or collapse. The terminology you may have heard — slipped disc, collapsed disc, crumbling spine — is almost always inaccurate and considerably more alarming than the reality warrants. Discs are not fragile structures, and neither are the nerve roots that run alongside them.
What can happen is that the outer casing of a disc, called the annulus fibrosus, develops a tear or weakness, allowing some of the softer inner material to bulge outwards. In some cases this creates enough pressure on a nearby nerve root to irritate it. But nerve roots are more resilient than most people realise. Even in the presence of disc change, there is usually enough space around the nerve root for it to accommodate. Many disc changes also reduce in size over time as the body naturally resorbs the material, which is part of why most people recover well without surgery.
Compression versus inflammation — and why it matters
This is a distinction that doesn’t get nearly enough attention in patient education, and it genuinely changes how we think about treatment.
Sciatica is sometimes caused by direct mechanical compression of a nerve root. But research is clear that many cases arise primarily from inflammation — the nerve root becomes chemically irritated and sensitised, without any significant mechanical pressure at all. In fact, inflammatory sciatica can produce pain that is just as severe as, or worse than compression-related sciatica. This has important implications for treatment: it helps explain why anti-inflammatory medication works well for many people, and it’s a significant part of the rationale for injection therapy directed at the nerve root.
It also explains something that often confuses people: the fact that pain severity doesn’t always match what a scan shows. A scan might reveal a relatively modest disc change while the pain is severe — because the inflammation, not the size of the bulge, is driving the experience. Conversely, a scan might show a large disc change in someone with minimal symptoms. A scan shows structure, not pain.
Other causes
Beyond disc-related changes, other causes of nerve root irritation include:
- Spinal stenosis — narrowing of the canals through which the nerve roots travel, which can result from bony changes, thickened ligaments, disc changes, or a combination of all; more common as people get older
- Spondylolisthesis — where one vertebra shifts forwards slightly relative to the one below it, which can narrow the space available for nerve roots
- Foraminal narrowing — specifically where the exit points (foramen) through which nerve roots leave the spine become restricted
- Piriformis syndrome / Deep gluteal syndrome — a less common cause where the nerve is compressed outside the spine by deep buttock muscles, though this is often over-diagnosed
Sciatica also affects people of all ages, though it’s most commonly seen in those in their forties and fifties. It can affect people doing physical jobs, people who sit for long periods, and everyone in between. There is no one ‘type’ of person who gets it.
How is sciatica assessed? What does a physiotherapy assessment actually involve?
Sciatica is fundamentally a clinical diagnosis — meaning a skilled physiotherapist can usually establish what’s going on from a thorough history and physical examination, without an immediate scan. Understanding what this assessment involves helps you know what to expect and why each part matters.
History taking
The assessment always begins with questions. Where exactly is the pain? What does it feel like — sharp, burning, electric, aching? Does it travel below the knee? What makes it better or worse? When did it start, and how has it behaved since? Is there any associated numbness, tingling, or weakness in the leg or foot?
The pattern and distribution of symptoms gives a great deal of clinical information. Each nerve root produces a characteristic distribution of symptoms — what we call a dermatomal pattern. Pain or numbness on the outer border of the foot, for example, typically points to the S1 nerve root. Symptoms extending to the big toe and top of the foot often suggest L5 involvement. Pain into the inner calf and altered sensation on the inside of the leg tends to point to L4. This level of detail guides the assessment and, ultimately, the treatment plan. However, it is worth noting that these dermatomal patterns can be slighlty differernt in everyone!
We also want to look at broader contributing factors — sleep quality, stress, activity levels, and general health are all genuinely relevant to how pain behaves and how quickly people recover. A good assessment doesn’t just look at the spine in isolation.
Physical examination
The physical examination will typically include several components:
- Neurological testing — assessing the strength of key muscle groups, sensation across the leg and foot, and deep tendon reflexes. The knee jerk reflex, for example, is associated with the L3 nerve root; the ankle jerk with S1. Changes in these reflexes can help to confirm which level is involved and whether the nerve is under enough pressure to be affecting its function.
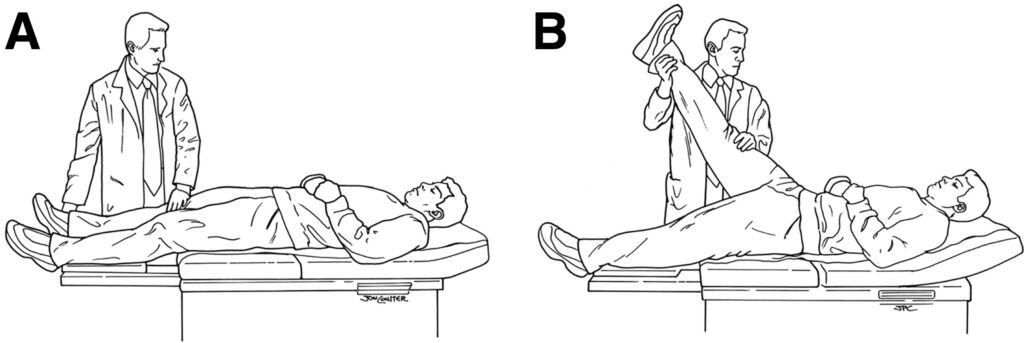
- The straight leg raise — one of the most well-known clinical tests for sciatica. With the patient lying flat, the leg is lifted with the knee straight, gradually tensioning the sciatic nerve. If this reproduces familiar leg pain at a relatively low angle of elevation — typically below 60 to 70 degrees — it’s a strong indicator of nerve root irritation. The test has good sensitivity, meaning it’s effective at identifying nerve root involvement when it’s present.
- Movement assessment and directional preference — observing how the spine moves in different directions, and identifying whether there is a specific direction of movement that reduces the leg pain. This is clinically important because it often guides the early rehabilitation programme. Some people find that certain extension-based movements ease the leg pain; others respond differently. Understanding this shapes the exercise prescription from the outset.
- Assessments of the areas around the spine is also important, for example, assessing the hip joint. It is possible to have more than 1 contributor of pain.
This combination of tests — history, neurological examination, and provocation tests — is usually sufficient to make a confident clinical diagnosis and begin treatment. The assessment tells us not just what’s going on, but what stage of recovery you’re at and which treatment approach is most appropriate for you right now.
Do you need a scan?
This is one of the most common questions I hear, and it’s understandable — when you’re in pain, it’s natural to want to know exactly what’s happening inside. But the honest answer, for most people with sciatica, is no — not straightaway, and often not at all.
Why scans are often not the first step
Sciatica is a clinical diagnosis — and in many cases, scans do not influence treatment plans. The management of sciatica in the early stages is the same regardless of what a scan shows: stay active, manage pain appropriately, engage with physiotherapy-guided rehabilitation, and allow time for the natural recovery process to work.
Requesting an MRI scan early in the course of sciatica also carries a risk that often goes undiscussed: the risk of over-interpretation. Degenerative changes in the spine are extremely common in the general population — in people of all ages, with and without symptoms — and finding them on a scan doesn’t necessarily mean they’re the cause of your pain.
What MRI scans show in people without any symptoms
This is where the research is really interesting, and where a lot of people find enormous reassurance once they understand it.
A landmark systematic review published in the American Journal of Neuroradiology looked at spinal imaging in completely pain-free individuals and found that degenerative changes were not only common — they were the norm. More than 50% of asymptomatic people in their thirties already showed disc degeneration, height loss, or disc bulging on MRI. By the age of 60, degenerative changes were present in nearly 90% of people who had no pain whatsoever.
To put some specific numbers on it: a well-cited study found that among people without any back pain:
- 52% had at least one disc bulge
- 27% had disc protrusions (what most people would think of as a “herniated disc”)
- At the L5-S1 level — the most commonly affected in sciatica — a herniated disc was visible in 35% of completely asymptomatic people over 50
The authors of the systematic review concluded that many of these findings are part of the normal ageing process rather than pathological processes requiring intervention. Disc degeneration, in other words, is to the spine what grey hair is to the scalp — a normal age-related change that doesn’t necessarily indicate a problem, and certainly doesn’t predict pain.
This matters because if you have an MRI and it shows a disc bulge or some degenerative change, that finding needs to be interpreted in the context of your actual symptoms and clinical examination — not in isolation. A report that lists degenerative findings can feel alarming if you read it without this context. A good physiotherapist or specialist can help you understand what’s relevant and what isn’t.
When imaging is appropriate
None of this means scans are never useful — far from it. There are specific situations in which imaging is clearly indicated:
- If there are any red flag symptoms — neurological deficit that is worsening, signs of cauda equina syndrome (see below), or suspicion of a serious underlying cause such as malignancy or infection
- If symptoms are severe and not responding to an adequate trial of conservative treatment — usually considered to be 6 to 12 weeks of well-managed physiotherapy and appropriate medication
- If surgery is being considered — in which case an MRI is essential for surgical planning, confirming the level and nature of nerve root compression
- If an injection is being considered — nerve root injection under imaging guidance requires knowing exactly which level to target, and an MRI is typically needed to inform that decision
- If the clinical picture is unclear — where the diagnosis isn’t straightforward or symptoms don’t follow an expected pattern, imaging can help resolve diagnostic uncertainty
MRI is the gold standard imaging choice for the lumbar spine and sciatic nerve pathology. It shows soft tissue structures — disc material, nerve roots, and the spaces they travel through — with far more detail than an X-ray. An X-ray shows bone and can rule out fractures or bony instability, but it cannot show disc changes or nerve root compression, and is rarely the right first investigation for sciatica.
Your physiotherapist can advise whether imaging is appropriate for your situation, and can make a referral if indicated — either directly or via your consultant.
Will sciatica get better on its own?
This is the question I’m asked more than any other, and the answer — for most people — is yes.
The natural history of sciatica associated with disc changes is actually quite favourable. Evidence shows that 60 to 80% of people see their symptoms resolve within 6 to 12 weeks, and at the one-year mark that figure rises to around 80 to 90%. Part of the reason is a process called disc resorption — the body’s immune system can actively break down and absorb herniated disc material over time, naturally reducing the pressure on the nerve root. It sounds remarkable, but it happens regularly and explains why many large disc herniations eventually settle without any intervention at all.
That said, recovery is rarely linear, and the early stages can be genuinely brutal. Pain can be severe, sleep is often disrupted, and it’s common to feel like you’re going backwards even when you’re not. The first four to six weeks tend to be the hardest. Things typically begin to shift after that, though the timeline varies considerably between individuals.
It’s also worth knowing that some factors can slow recovery down. Research has identified prolonged sitting or driving, physically demanding work, high levels of distress, and long symptom duration before treatment as factors associated with a slower or more complicated recovery. None of these are insurmountable — but being aware of them helps to set realistic expectations and tells us where to focus energy in treatment.
What does recovery actually feel like?
One of the most commonly misunderstood parts of sciatica recovery is what improvement actually looks and feels like — because it doesn’t always feel like getting better.
A well-recognised pattern of recovery is called centralisation. As the nerve root calms down, the pain tends to gradually retreat up the leg — moving from the foot, to the calf, to the thigh, and eventually into just the back — before it finally resolves. People often experience this as the pain “moving around” or worry that it’s getting worse. In almost all cases it isn’t. Centralisation is a good sign, and it’s something your physiotherapist will be looking for during reassessment.
Numbness, tingling, and altered sensation in the leg or foot can persist even after the pain has settled significantly. Nerve tissue heals more slowly than muscle or tendon. It’s also more sensitive to mechanical loading, which is why sensory symptoms are often the last to resolve. If you’ve had numbness for several weeks, it doesn’t mean the nerve has been permanently damaged — it usually means it’s still on its way back to normal. Patience is required, and it can feel frustrating, but continued progress in function and pain is reassuring even when sensation takes longer to normalise.

Exercise and rehabilitation: what actually helps
The evidence base for specific exercise types in sciatica is genuinely challenging — the research is heterogeneous, the populations studied are varied, and systematic reviews acknowledge that no single exercise type has emerged as clearly superior. What is consistent across guidelines and clinical experience is this: keeping active, in a managed and progressive way, is better than rest. And working with a physiotherapist who can tailor the approach to your specific presentation is considerably better than generic advice.
Keep moving — but move well
Bed rest has been consistently shown to offer no benefit over staying active in sciatica, and in practice tends to make things worse — both physically, by allowing deconditioning and increasing pain sensitivity, and psychologically, by reinforcing fear and avoidance of movement. The goal early on is not to find a position and stay in it, but to keep exploring movement within what’s tolerable.
Walking is one of the most accessible and often one of the most helpful things you can do in the early stages. Even short distances, done regularly, help to maintain function, manage inflammation, and preserve confidence in your ability to move. Swimming is another option that many people find well-tolerated. There is no single ‘best’ exercise for sciatica — the most important thing is choosing activity you can actually stick to.
Nerve mobilisation
Nerve mobilisation techniques — often called neural flossing or nerve gliding — involve gentle, rhythmic movements that encourage the sciatic nerve to move freely through the surrounding soft tissues. When a nerve has been irritated, it can become sensitised and mechanically restricted, and these techniques aim to restore its normal movement.
Done correctly, nerve mobilisation can help to reduce the tightness, sensitivity, and pulling sensation that often accompanies sciatica. These are not aggressive stretches — they’re subtle, controlled movements, and the intensity and approach will be guided carefully by your physiotherapist based on your current symptom level. They’re typically introduced once the acute phase has settled enough to tolerate them.
Progressive loading and long-term rehabilitation
As pain begins to settle and function improves, rehabilitation shifts focus from symptom management to rebuilding capacity. This means progressively increasing strength, particularly in the lower back, gluteal, and leg muscles — not because weakness caused the sciatica, but because building strength and resilience reduces the risk of recurrence and restores full function.
This phase of rehabilitation is where a structured, progressively loaded programme makes a real difference. Strengthening/resistrance training and endurance work are all relevant here. The goal is not just to get you out of pain, but to get you back to doing the things that matter — sport, work, sleep — with confidence.
What about medication?
Medication has a useful role in sciatica, primarily in the acute and subacute phases — helping to bring pain down to a level where you can move, sleep, and engage with rehabilitation. It doesn’t treat the underlying cause, but it can make a real difference to your quality of life while the natural recovery process does its work. Here’s a plain-language guide to the main options and what the evidence actually says about each.
NSAIDs (anti-inflammatory medication)
Non-steroidal anti-inflammatory drugs — ibuprofen, naproxen, diclofenac, and others — are typically the first medication to try. They work by reducing the inflammatory component of nerve root irritation, and for many people they provide meaningful relief in the early stages. They’re most effective when taken regularly at an adequate dose for a defined period rather than sporadically as needed, ideally with food to protect the stomach lining.
NSAIDs are not suitable for everyone. People with a history of peptic ulcer disease, significant kidney problems, or certain cardiovascular conditions may be advised against them. If you’re unsure whether they’re appropriate for you, check with a healthcare professional before starting them.
Amitriptyline
Amitriptyline is a tricyclic antidepressant, but at the low doses used for nerve pain — typically 10 to 30mg — it’s being used for an entirely different purpose. At these doses, amitriptyline works on the way the nervous system processes and amplifies pain signals, modulating the neuropathic element of sciatica: the burning, shooting, electric-feeling pain that comes from nerve root irritation.
It’s usually taken at night because it can cause drowsiness — which can actually be helpful for people whose sleep is being disrupted by pain. NICE recommends it as one of the first-line options for neuropathic pain, and it has a long track record of use in this context. It typically takes one to two weeks to begin noticing an effect on pain.
Duloxetine
Duloxetine is a serotonin-norepinephrine reuptake inhibitor (SNRI) antidepressant with well-established evidence for neuropathic pain, and it’s similarly recommended by NICE as a first-line option alongside amitriptyline. It’s generally taken during the day, tends to be better tolerated than amitriptyline by some people — particularly those who find the drowsiness side effect problematic — and typically takes a few weeks to build to its full effect.
Both amitriptyline and duloxetine are used for their pain-modulating properties in sciatica, not for their antidepressant effects. This is worth emphasising because patients are sometimes surprised — or concerned — to be offered an antidepressant for back and leg pain. The dose and the mechanism of action are entirely different to their use in depression.
A word on gabapentin and pregabalin
This section is worth reading carefully, particularly if you’ve already been prescribed one of these drugs.
Gabapentin and pregabalin are very widely prescribed for sciatica, and yet the NICE guideline on low back pain and sciatica is unambiguous: these drugs should not be offered for sciatica. The evidence review found no meaningful clinical benefit specific to sciatica, and the committee were clear that the harms outweigh the benefits for most people. Those harms include dizziness, cognitive impairment, fatigue, sedation, and a significant risk of dependence — which is why both drugs are now classified as Schedule 3 controlled substances in the UK.
If you are currently taking gabapentin or pregabalin for sciatica and they aren’t helping, it’s worth discussing this with your prescribing healthcare professional. Stopping these medications should be done gradually — abrupt withdrawal can cause significant side effects — so this should be managed with appropriate support.
Similarly, opioid medications are not recommended for chronic sciatica. While they may have a very limited short-term role in severe acute pain, the evidence for their use in ongoing sciatica management is poor and the risks — dependence, tolerance, and a range of side effects — are well-documented.
When is an injection worth considering?
For some people with sciatica, pain levels remain high enough — despite appropriate medication and physiotherapy — that engaging meaningfully with rehabilitation feels close to impossible. Functioning at work is difficult. Sleep is severely disrupted. Sitting for any length of time is unbearable. This is where an injection can meaningfully change the trajectory of recovery.
What does a nerve root injection involve?
The most commonly used approach for sciatica is an epidural steroid injection — and more specifically, a selective nerve root injection, which delivers corticosteroid medication as close as possible to the affected nerve root. Given that inflammation plays such a central role in many cases of sciatica, delivering targeted anti-inflammatory treatment directly at the source makes considerable clinical sense. Evidence from multiple systematic reviews supports nerve root injections being superior to placebo for reducing leg pain in the short term.
The aim of the injection is not to cure the underlying problem — it’s to significantly reduce nerve root inflammation, creating a window of substantially lower pain in which rehabilitation can happen far more effectively. Injection and physiotherapy, in other words, are complementary — the injection doesn’t replace rehabilitation, it enables it.
This is a straightforward outpatient procedure carried out under imaging guidance — typically fluoroscopy (live X-ray) — to ensure accurate placement of the medication. There’s no surgery involved, no general anaesthesia, and most people are back to their usual activities within a day or two. The majority of people notice a meaningful improvement in leg pain within one to two weeks of the injection.
Who is an injection appropriate for?
Injections are not for everyone, and they’re not always necessary. They’re most appropriate where:
- Leg pain is the dominant symptom and is significantly affecting function or quality of life
- Conservative management — adequate medication and structured physiotherapy — has not produced enough improvement
- An MRI has confirmed the level and nature of nerve root involvement, allowing accurate targeting
- There are no contraindications such as active infection, certain blood-thinning medications, or uncontrolled diabetes
In my practice, when sciatica isn’t responding adequately to conservative management, I refer patients to a specialist spinal consultant for nerve root injection under imaging guidance. The two approaches — injection and physiotherapy — work best together, and I work with patients to ensure the rehabilitation programme is in place and ready to build on the relief the injection provides.
Is surgery ever needed?
For the majority of people, the answer is no — and this is worth stating clearly, because surgery is often a source of significant anxiety.
Surgery for sciatica — typically a microdiscectomy, where the portion of the disc pressing on the nerve root is removed — is generally considered when symptoms are severe and have not responded to an adequate trial of conservative treatment, or when there is progressive neurological deficit. Evidence suggests that surgery produces faster relief than conservative treatment in the short to medium term for those with significant disc herniation — but at one year, outcomes are broadly similar between surgical and non-surgical management in many cases. The body, given time and the right support, is often capable of achieving the same result without an operation.
Surgery becomes more urgent — and should not be delayed — if there are signs of significant and worsening neurological compromise, or any suggestion of cauda equina syndrome. Your physiotherapist will discuss the surgical pathway with you if it becomes relevant, and can advise on appropriate specialist referral.
When should you seek urgent help?
Most sciatica, while extremely painful, is not a medical emergency. There are, however, a small number of symptoms that require same-day urgent assessment. Please seek immediate medical attention — via A&E or 999 if necessary — if you develop any of the following alongside your back and leg pain:
- Numbness or tingling in the saddle area — the groin, inner thighs, or buttocks
- Loss of bladder or bowel control, or difficulty passing urine
- Rapidly worsening weakness in one or both legs
These symptoms can indicate cauda equina syndrome — a rare but serious condition in which the bundle of nerve roots at the base of the spinal cord is significantly compressed. It requires emergency assessment and, where confirmed, urgent surgical decompression. If you experience any of these symptoms, do not wait to see if they improve — seek help immediately.
When is it worth seeing a specialist physiotherapist?
You don’t need to wait until things become unbearable. If your leg pain is severe, hasn’t started to improve after a few weeks of conservative management, or is significantly affecting your sleep, work, or daily life — getting an expert assessment sooner rather than later is worth it.
A specialist MSK physiotherapy assessment gives you clarity: what’s driving your symptoms, where you are in the recovery process, what treatment approach is right for you at this stage, and what to expect. It’s the difference between a generic set of exercises from a leaflet and a treatment plan built around your specific presentation.
For some people that plan involves mainly reassurance, education, and a targeted home exercise programme. For others it involves hands-on treatment, progressive rehabilitation, onward referral for imaging, or advice and referral for injection therapy. The right approach depends entirely on the individual — which is why the assessment comes first.
Ready to get your recovery on track?
Sciatica can feel relentless — particularly in those first brutal weeks. But with the right management and the right support, the vast majority of people do get through it. If you’d like a specialist assessment, feel free to get in touch or book a consultation directly. We’ll get to the bottom of what’s going on and put a plan together that’s built around you.