

Table of Contents
So What’s Actually Going On?
You’ve got muscles in your buttock — called the gluteus medius and gluteus minimus — that attach to the bony bit on the outside of your hip (the greater trochanter). The tendons that connect those muscles to the bone can become irritated and painful over time. That’s what gluteal tendinopathy is — the tendon is unhappy because of how it’s being loaded.
The reason the “bursitis” label matters is that it implies inflammation that needs calming down. But research has shown that true inflammation in this area is actually pretty rare. The real issue is the tendon. And when you know that, it changes the whole approach to treatment — because what helps a tendon is quite different to what helps inflammation.
However in practice, we tend to use the terms gluteal tendinopathy and greater trochanter pain syndrome interchangeably. Although gluteal tendinopathy is the more modern label, many patients (and healthcare professionals) still term this pain greater trochneric pain syndrome, or GTPS for short.
How Common Is It?
Really common. It’s actually the most common tendon problem in the lower body. Up to 23.5% of women and about 8.5% of men between the ages of 50 and 79 are affected (Grimaldi et al., 2024). Women get it about four times more often than men, and it’s especially common around and after the menopause.
One thing that surprises people is just how much it can get in the way of normal life. Research has found that the levels of pain and disability are similar to those waiting for a hip replacement. It can mess with your sleep, make walking uncomfortable, and take the enjoyment out of things you used to do without thinking. So if it’s been getting you down — that’s completely understandable. This isn’t something minor, and it doesn’t tend to just go away on its own.
What Causes It?
It’s rarely one thing. Usually it’s a combination of factors:
Doing too much, too quickly. A big weekend of walking, a new gym class, or even just a lot more stairs than normal can be enough to overload the tendon. Going from not very active to suddenly doing loads is one of the most common triggers.
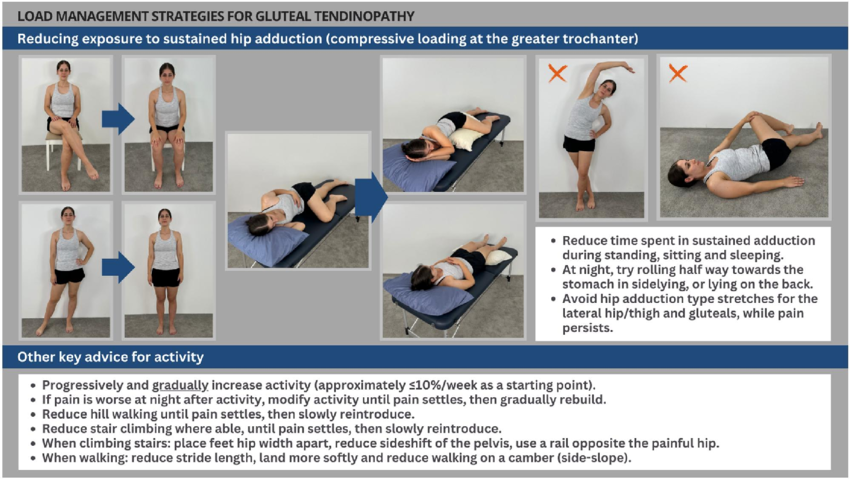
Compression. This one’s important. The tendons get squashed against the bone when your hip moves inward. Things like crossing your legs, standing with all your weight on one hip, sitting in low chairs, or lying on your side without a pillow between your knees all increase that compression.
Hormonal changes. Oestrogen helps keep tendons healthy. When oestrogen levels drop during and after the menopause, tendons can become weaker and slower to repair. That’s a big part of why this condition is so common in women going through that stage of life.
Weak glute muscles. People with gluteal tendinopathy often have noticeable weakness in the hip muscles — sometimes on both sides, even when the pain is only on one. That weakness changes the way you walk and move, which puts even more strain on the tendons.
Other things like carrying extra weight, conditions such as diabetes or high cholesterol, getting older, the shape of your hip bones, and even certain antibiotics can play a part too.
Things That Make It Worse
I know this bit can feel a bit overwhelming, but honestly, a few simple tweaks to your day-to-day habits can make a surprisingly big difference. Here’s what to watch out for: crossing your legs when sitting; hanging on one hip when standing (you know the stance — hip popped out to one side); sleeping on your side without a pillow between your knees; and one that catches a lot of people out — stretching the outside of the hip. It feels like it should help, but those ITB and glute stretches actually squash the tendon more. Best to avoid them while things are sore.
Try not to ramp up your activity too fast either. A rough guide is no more than about 10% increase per week. And here’s the thing — complete rest doesn’t work for tendons. They actually need some load to get better. It’s just about getting the right amount.
What Actually Works?
Here’s where things get encouraging. The research has come a long way, and we now have a clear picture of what works best.
Education and exercise is the number one approach. A big, high-quality trial called the LEAP trial compared physiotherapy-led education and exercise against a steroid injection and a wait-and-see approach. The exercise group came out on top — better outcomes at 8 weeks and at one year (Mellor et al., 2018). That’s since been backed up by a 2025 systematic review confirming meaningful improvements in both pain and function. In practice, this usually starts with simple exercises — like gently pressing your leg outward against resistance without moving it — and builds toward heavier strengthening over time. Alongside the exercise, you’ll learn how to manage the load on your tendon day to day.
In the LEAP trial, 77% of the exercise and education group rated themselves as at least moderately better by 8 weeks, and 78% at one year. That’s a solid success rate for a non-invasive approach.
What About Shockwave Therapy and Steroid Injections?
These are two questions that come up all the time in clinic, so let me walk you through both.
Shockwave therapy uses focused sound waves delivered through the skin into the affected tendon. It’s not as scary as it sounds — it’s a handheld device pressed against the outside of your hip, and each session takes about ten minutes.
Where shockwave really comes into its own is when your hip isn’t massively irritable but the tendon just isn’t responding to exercise alone. Think of it as something that helps alongside your rehab, not instead of it. It can help settle the tendon down and create a better environment for the strengthening work to take effect. A recent systematic review found that shockwave therapy showed better long-term results than steroid injection. It’s typically done as a course of three to five sessions, spaced about a week apart, and fits well into a broader rehab plan. Find more information here.
Steroid injections get a bit of a mixed reputation, and that’s partly deserved. The injection is a way for a very targetted anti-inflammatory medication to be delivered to a target sructure. The honest truth is they’re not a long-term fix on their own — at one year, people who had a steroid injection did no better than those who just waited it out (Grimaldi et al., 2024). There’s also evidence that corticosteroids can have negative effects on tendon tissue, reducing cell health and collagen quality.
But — and this is important — there are times when a steroid injection can be genuinely helpful for this gluteal pain. If your pain is really high and it’s stopping you from sleeping or walking properly, sometimes you need to bring things down before you can start the exercises that will help long term. A well-timed injection can take the edge off enough to let you engage with your rehab. The key is using it as a window of opportunity, not a solution in itself. Without the right exercise and load management afterwards, the pain will almost certainly come back once the effect wears off. Find more information here.
So in short: exercise and education first. Shockwave can be a great add-on when progress has plateaued. And a steroid injection can be a useful tool when pain is really high and stopping you from getting started with rehab.
When Should You Get It Looked At?
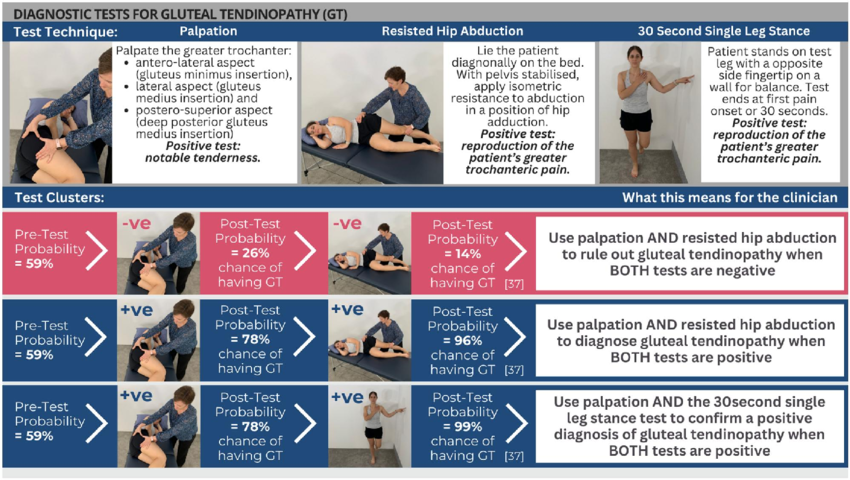
If you’ve had pain on the outside of your hip(gluteal/buttock) for more than a few weeks and it’s getting in the way of sleep, walking, or the things you enjoy — get it checked out. Hip pain can come from a few different places, including the hip joint itself or the lower back, so getting the right diagnosis matters. A specialist MSK physiotherapist can usually work out what’s going on through a good clinical assessment — most people don’t need a scan to get started on the right path.
Ready to Get on Top of Your Hip Pain?
If any of this sounds like you, your physiotherapist can help you figure out what’s going on and put together a plan to get you feeling better — whether that’s a progressive exercise programme, practical load management advice, or looking at shockwave or injection therapy where needed. Book a consultation with Bradley Rugg at bradleyrugg.co.uk for a thorough assessment and a plan tailored to you and your gluteal pain. You don’t have to just put up with it.